
Hyponatremia
Definition: Na < 135meq/L
Symptoms: Muscle cramps, headaches, falls, confusion, altered mental status, coma, and seizures.
General Info: These symptoms can lead to prolonged ICU and hospital days. Identifying the underlying cause and correcting the underlying cause can help the patient. Below is a quick way to breakdown hyponatremia to make sure it is getting evaluated and treated.
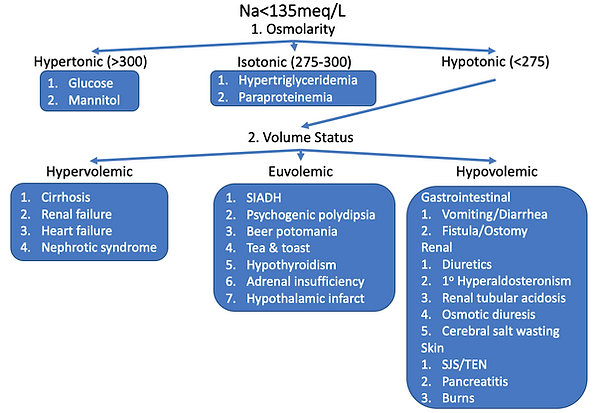
Differential: There are two branch points when breaking down hyponatremia. One is a lab value and one is a physical exam finding. This helps divide hyponatremia into its 5 subcategories.

The two branch points are osmolarity and volume status. This creates the 5 subcategories for hyponatremia.

5 Subcategories of Hyponatremia
-
Hypertonic Hyponatremia
-
Isotonic Hyponatremia
-
Hypotonic Hypervolemic Hyponatremia
-
Hypotonic Euvolemic Hyponatremia
-
Hypotonic Hypovolemic Hyponatremia
Why is it important to narrow down the hyponatremia to one of these subtypes?
It will help with the management of the patient.
The first differential to look at is hypertonic hyponatremia. It helps if you know the serum osmolarity equation.

This differential will be substances in the blood that increase osmolarity that are not sodium. The most common being glucose. There is a correctional factor for hyperglycemia so that you know what the sodium would be when the glucose is corrected. For every 100 above 100mg/dL of glucose add 1.6meq of Na. another osmotically active cause is mannitol. BUN and ethanol are unique in that they contribute to measured osmolarity but not effective osmolarity (tonicity). This is why they are not included in this list and it is important to understand in terms of risk for hyponatremia symptoms.

The next group is isotonic hyponatremia. It is based on substances in the blood that are not osmotically active but are proteins and fats and will dilute the serum sodium. This group is also called pseudohyponatremia because it is a lab finding and not truly hyponatremia. This group includes hypertriglyceridemia and paraproteinemia. I have been told that in order for a triglyceride level to be elevated enough to cause hyponatremia the blood will have a milky color. Paraproteinemias include MGUS and multiple myeloma.

The last osmolarity group is hypotonic hyponatremia which is the most common osmolarity category we see. It is also split into 3 categories, and is based on volume status.

The first group of hypotonic hyponatremias is hypervolemic. These are disease processes where the patient has gained water and salt but more water than salt. They include renal failure, liver failure, heart failure and nephrotic syndrome.

The second group is euvolemic hypotonic hyponatremia. These people have a wide differential. The most well-known is syndrome of inappropriate ADH (SIADH). The other unique ones are psychogenic polydipsia, beer potomania, and tea & toast. There is also hypothyroidism, adrenal insufficiency and a hypothalamic infarct.

The final group is hypovolemic hypotonic hyponatremia. You can also make a branch point within this group if it helps. These people have lost water and salt but lost more salt than water. Anytime fluid is lost from the body it can only be lost three ways; kidneys, GI tract, and skin. There is technically a fourth category, which is artificially with dialysis. This third branch point is based on this. Causes due to the GI tract are diarrhea, vomiting, fistulas and ostomies. Kidney losses are primary hyperaldosteronism, renal tubular acidosis, osmotic diuresis, and cerebral salt wasting. A common cause of hypovolemic hypotonic hyponatremia is due to diuretic use. The last group of disease is secondary to loss through the skin including TEN, Steven-Johnson syndrome, and burns.
Work-up: The initial work up is done with by sending serum osmolarity to help find the subcategory. The urine sodium, urine creatinine, and urine osmolarity is used to distinguish between renal and extra-renal causes. Urine urea can be sent if the patient is on diuretics and FeUrea calculated.

Management: If the patient is symptomatic give hypertonic saline. This is typically only seen
when the patient has sodium, <120meq/L. If the patient is not symptomatic then the best overall treatment is to treat the underlying condition. If it is chronic hyponatremia then correcting too fast can cause osmotic demyelination and should not be corrected more than 8meq/L in 24hours. If it is acute, the correction can be faster, but it is often done at around the same rate for precaution.
Hyponatremia is only worrisome if it is hypotonic. It is the hypotonicity that can cause diffusion of water intracellular and cerebral edema leading to life-threatening symptoms. It is worth noting, as stated earlier, that ethanol and uremia can increase measured osmolarity, but since it does not change tonicity, the patient is still hypotonic hyponatremia and should be treated as such.
For hypotonic hyponatremia, additional treatment is based on the volume status. In hypervolemic hypotonic hyponatremia, the treatment is fluid restriction and diuresis, usually loop diuretics. The treatment for hypovolemic hypotonic hyponatremia is by giving salt-containing fluids.
The nuance comes with the treatment for euvolemic hypotonic hyponatremia. For this group, the default is to fluid restrict. This is done in case it is SIADH. When a patient has SIADH the urine osmolarity is often higher than the osmolarity of the crystalloid solution given to the patient. This causes free water to be left in the body in order to meet the urine osmolarity of SIADH and actually worsens hyponatremia.

If SIADH is ruled out, IV salt solutions can be given. If SIADH is not ruled out, you can give a salt
solution with a higher osmolarity than the urine osmolarity of the patient.
Disposition: If the hyponatremia is mild or chronic then the patient should be discharged with follow up. If it is acute or a significant drop then the patient should be admitted for further work-up. If it is severe, <120meq/L, or symptomatic then there should be consideration for admission to the ICU.
Resources:
-
Blogs/Podcasts/Videos:
-
FizzICU.com: Hyponatremia: Time to be more specific
-
-
Lectures/Handouts:
-
References: